
Antiphospholipid Syndrome
Patients with persistent anti-phospholipid (aPL) antibodies and thrombosis or pregnancy-related morbidity are diagnosed with the autoimmune disorder antiphospholipid syndrome (APS). Official classification criteria for APS recognize three distinct, but overlapping aPL populations: antibodies against the phospholipid (PL)-binding protein β2-glycoprotein I (β2GPI), antibodies against β2GPI bound to cardiolipin and antibodies that prolong clotting times in a PL-dependent manner; so called lupus anticoagulant (LAC). The persistent presence of one or more of these antibody populations in patients with thrombosis or pregnancy morbidity is sufficient for the diagnosis of APS
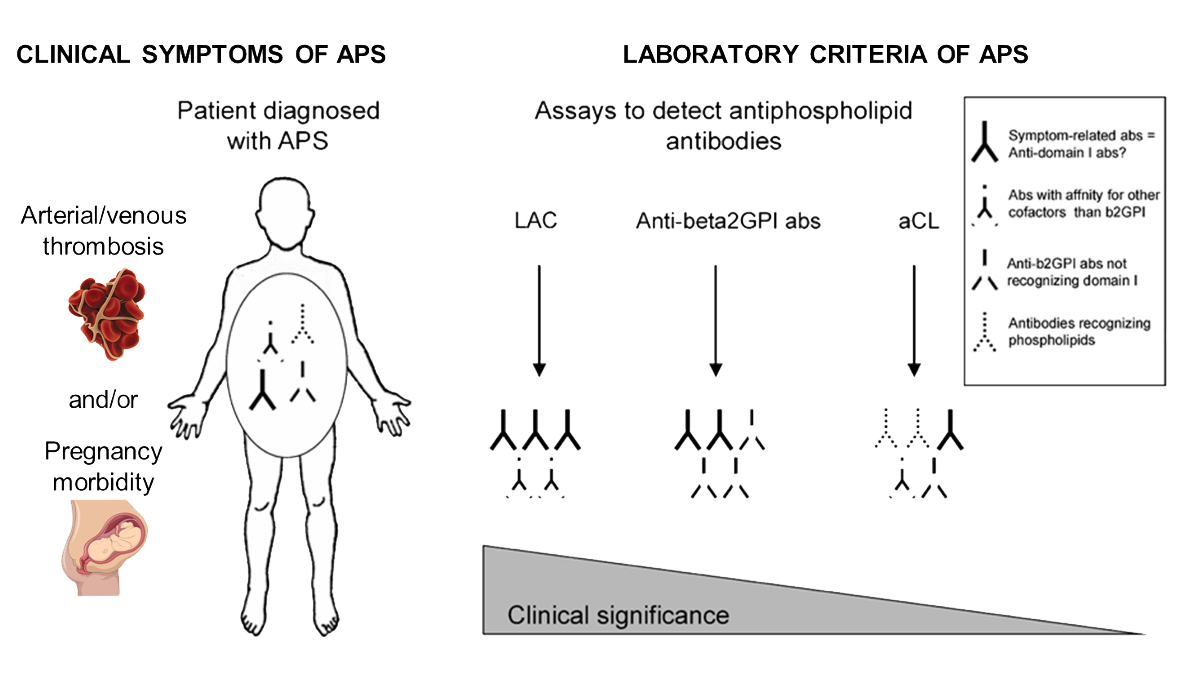
More and more evidence exists that the primary antigenic target of aPL is PL-bound β2GPI. This plasma glycoprotein circulates at a high concentration, but its physiological function is unknown. There is ample evidence that the presence of antibodies against β2GPI that display LAC activity is associated with a higher risk of thrombosis than the presence of other aPL. β2GPI has been shown to exist in different conformations, an ‘open’ and ‘closed’ conformation. A conformational change induced by interaction with anionic surfaces is mandatory for the exposure of the pathogenic epitope G40-R43 on domain I and hence to enable anti-β2GPI antibodies to interact with the epitope. Antibodies against this epitope correlate with an increased risk for thrombosis. By detecting only these “anti-domain I” antibodies the false positive rate reduces, resulting in an increased specificity. Interestingly, we have demonstrated clear differences in exposure of epitope G40-R43 on domain I of β2GPI in commercially available anti-β2GPI IgG assays. Importantly, we found that a significant number of samples positive for domain I reactivity are falsely assigned negative in assays characterized by a decreased availability of this epitope. The detection of anti-β2GPI and anti-cardiolipin antibodies for the diagnosis of the antiphospholipid syndrome (APS) is mainly done by quantitative endpoint assays.
Taking into account that not all antibodies directed against β2GPI and cardiolipin/β2GPI are pathogenic, such non-functional assays result in a relatively high false positivity. Probably due to the fact that LAC measures a functional effect of the antibodies, LAC is a better predictor of thrombosis than quantitative solid-phase immunoassays. However, the specificity and sensitivity of LAC largely depend on the calculation of cut-off values, the choice of the reagents and a number of uncertainties exist in the interpretation of the results. Despite differences in risk profile associated with the aPL subtypes, all APS patients currently receive the same treatment to prevent recurrence of thrombotic events: life-long antithrombotic therapy with vitamin K antagonists. Treatment with these drugs is associated with a high risk of potentially life-threatening bleeding complications. Hence, there is an urgent need for a means to discriminate between patients at risk for thrombosis versus patients not at risk for an event. Current available diagnostic tools fail to make this distinction. Therefore, we believe the optimization of a functional assay, such as a thrombin generation-based assay, for the diagnosis of APS and the prediction of thrombosis is warranted.
1. Miyakis S, Lockshin MD, Atsumi T, Branch DW, Brey RL, Cervera R, Derksen RH, DE Groot PG, Koike T, Meroni PL, Reber G, Shoenfeld Y, Tincani A, Vlachoyiannopoulos PG, Krilis SA. International consensus statement on an update of the classification criteria for definite antiphospholipid syndrome (APS). J Thromb Haemost. 2006;4(2):295-306.
2. Pelkmans L, de Laat B. Antibodies against domain I of beta2-glycoprotein I: the one and only? Lupus. 2012 Jun;21(7):769-72.
3. de Laat B, van Berkel M, Urbanus RT, Siregar B, de Groot PG, Gebbink MF, et al. Immune responses against domain I of beta(2)-glycoprotein I are driven by conformational changes: domain I of beta(2)-glycoprotein I harbors a cryptic immunogenic epitope. Arthritis and rheumatism. 2011;63(12):3960-8.
4. de Laat B, Pengo V, Pabinger I, Musial J, Voskuyl AE, Bultink IE, et al. The association between circulating antibodies against domain I of beta2-glycoprotein I and thrombosis: an international multicenter study. Journal of thrombosis and haemostasis : JTH. 2009;7(11):1767-73.
5. Pelkmans L, Kelchtermans H, de Groot PG, Zuily S, Regnault V, Wahl D, et al. Variability in exposure of epitope G40-R43 of domain i in commercial anti-beta2-glycoprotein I IgG ELISAs. PloS one. 2013;8(8):e71402.
6. Devreese K, Hoylaerts MF. Laboratory diagnosis of the antiphospholipid syndrome: a plethora of obstacles to overcome. European journal of haematology. 2009;83(1):1-16.